

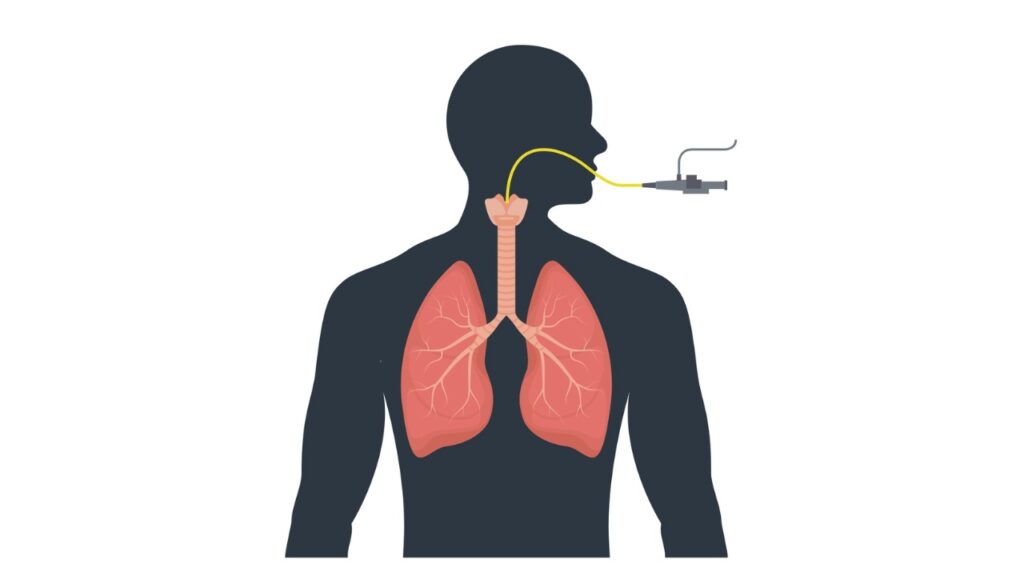



Capnography may be the most important vital sign you use to monitor your EMS patient. It provides
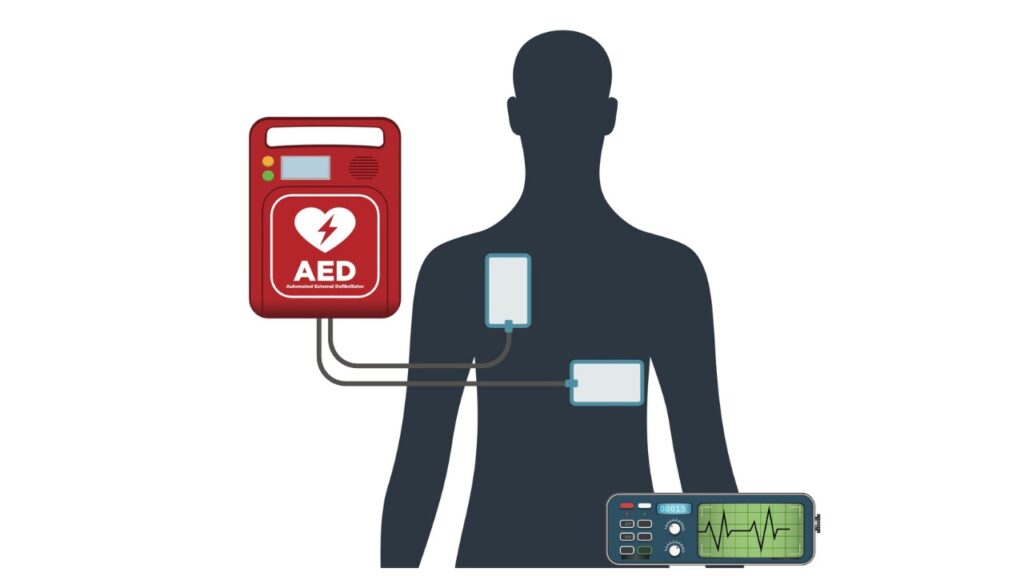
Imagine your patient presents with no pulse. You begin CPR and hook the patient up to your
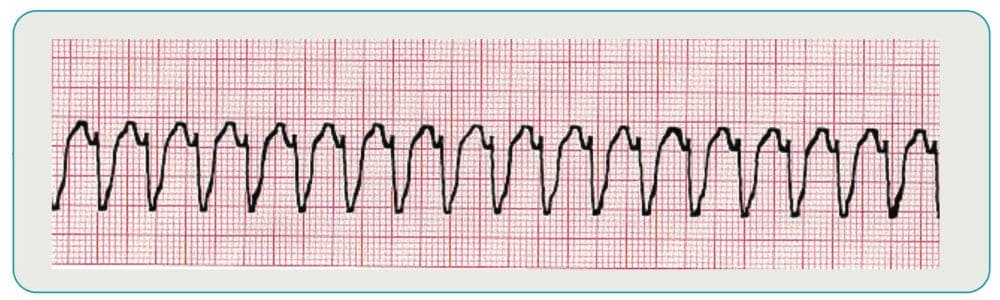
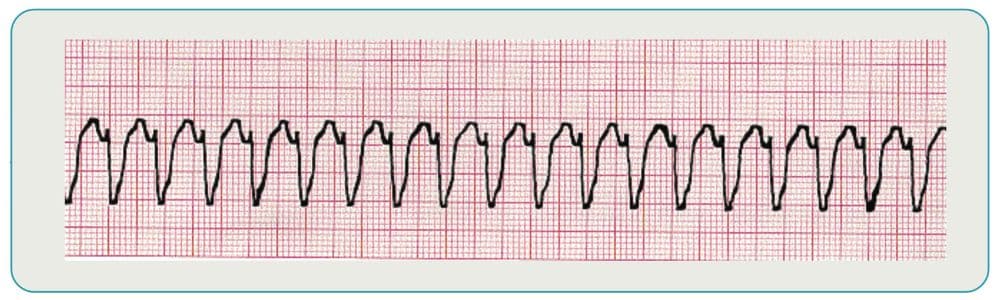
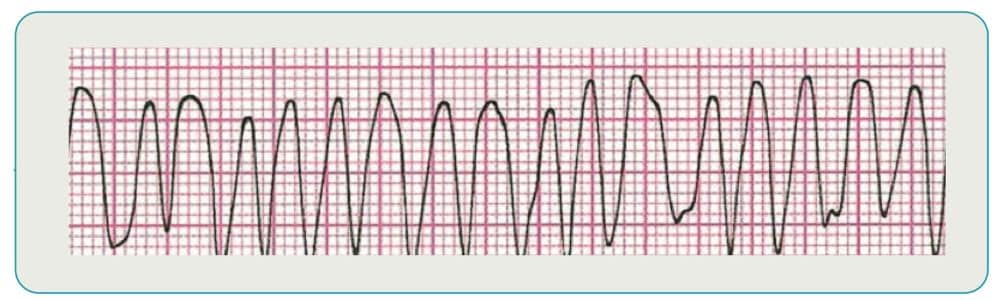
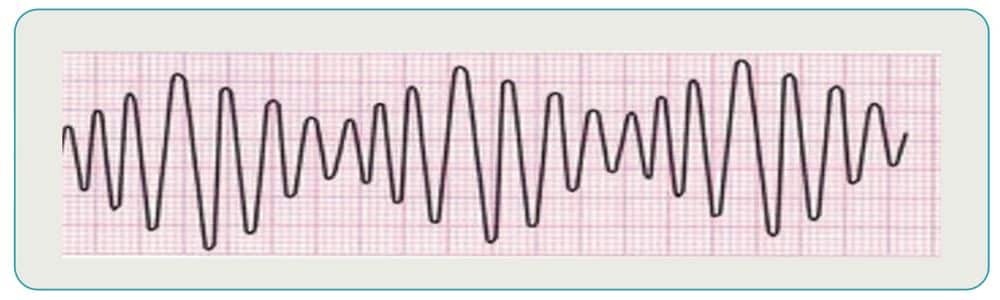
Ventricular tachycardia (Vtach) and ventricular fibrillation (Vfib) are two potentially life-threatening heart arrhythmias that originate in the



